When someone has a stroke, every second counts. But not all strokes are the same. Two main types - ischemic and hemorrhagic - happen for completely different reasons, need totally different treatments, and require unique prevention strategies. Knowing the difference isn’t just medical jargon; it can save a life.
What Exactly Is a Stroke?
A stroke happens when the brain doesn’t get enough blood. Brain cells start dying within minutes without oxygen. The result? Loss of movement, speech, vision - or worse. About 795,000 people in the U.S. have a stroke every year. One in 19 deaths is from stroke. That’s more than breast cancer and prostate cancer combined.Ischemic Stroke: The Blockage
This is the most common kind - about 87% of all strokes. It happens when a clot blocks a blood vessel feeding the brain. Think of it like a clogged pipe. The clot can form right in the brain, or it can travel from elsewhere - like the heart. There are three main types of ischemic strokes:- Thrombotic strokes: A clot forms inside a brain artery. This often happens because of plaque buildup from atherosclerosis. About half of all ischemic strokes fall into this category.
- Embolic strokes: A clot forms somewhere else - usually the heart - and travels to the brain. This is common in people with atrial fibrillation (AFib), where the heart beats irregularly and lets blood pool and clot.
- Cryptogenic strokes: No clear cause is found after testing. These make up about 30% of ischemic strokes. They’re frustrating, but research is improving how we find hidden causes.
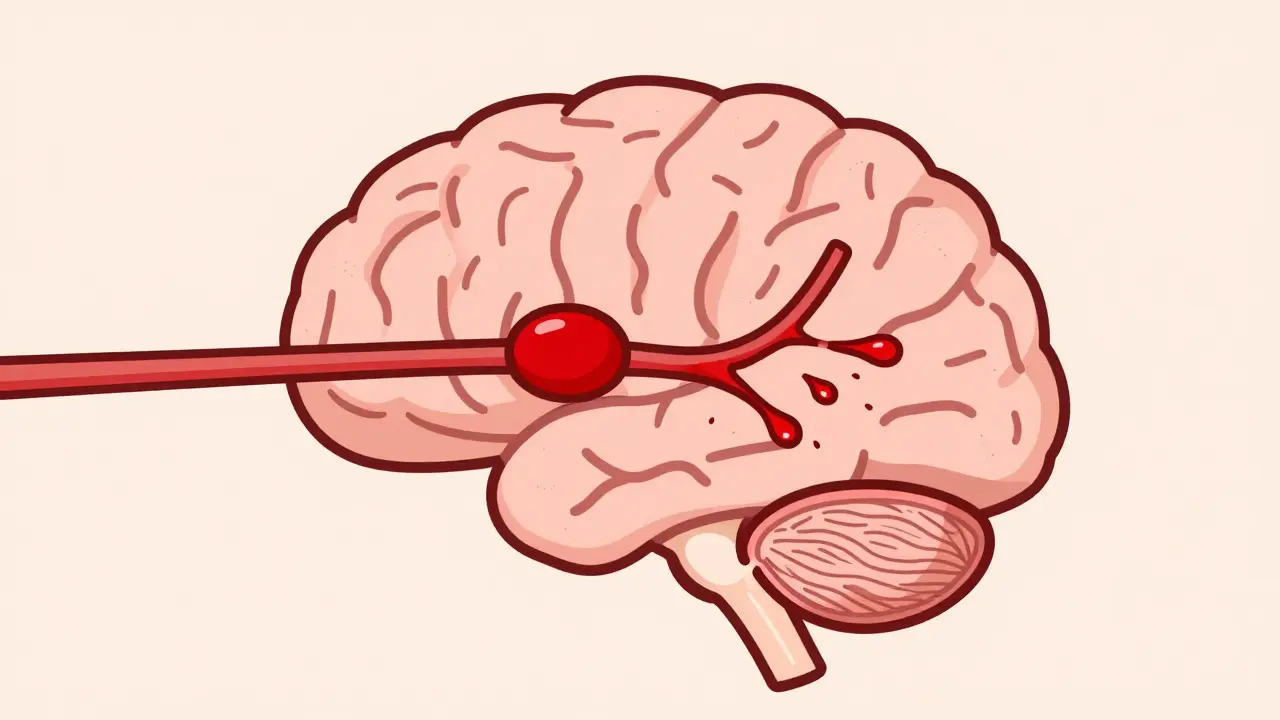
Hemorrhagic Stroke: The Burst
This type is less common - only 13% to 15% of strokes - but often more deadly. Instead of a blockage, a blood vessel bursts inside or around the brain. The pressure from the leaking blood crushes brain tissue. There are two main kinds:- Intracerebral hemorrhage: A vessel bursts inside the brain tissue. This is most often caused by long-term high blood pressure. About 78% to 88% of these cases are linked to uncontrolled hypertension.
- Subarachnoid hemorrhage: A vessel on the brain’s surface ruptures, usually because of a burst aneurysm. This is the kind that comes with a sudden, extreme headache - often described as "the worst headache of my life." It’s rare but dangerous.
How Do the Symptoms Differ?
Both types cause sudden problems like numbness, confusion, trouble speaking, or weakness on one side of the body. But hemorrhagic strokes often hit harder and faster. Here’s what sets them apart:- Headache: 92% of hemorrhagic stroke patients report a sudden, severe headache. Only 19% of ischemic stroke patients do.
- Seizures: Happen in 17% of hemorrhagic cases. Almost never in ischemic.
- Eye changes: Dilated pupils, unequal pupils, or trouble moving the eyes are far more common in hemorrhagic strokes.
- Agitation: Nearly 80% of hemorrhagic stroke patients show signs of confusion or agitation. Only 7% of ischemic cases do.
Treatment: Why Speed and Type Matter
Time is brain - and the treatment depends entirely on the type. For ischemic strokes, doctors try to dissolve or remove the clot. The gold standard is a drug called alteplase (tPA), given within 3 to 4.5 hours of symptom onset. A newer option, tenecteplase, is now approved and works just as well, with fewer side effects. For large clots in major brain arteries, a mechanical thrombectomy - a procedure where a device physically pulls the clot out - can be done up to 24 hours after symptoms start. Studies show this improves recovery by 40% compared to medication alone. For hemorrhagic strokes, you can’t give clot-busting drugs - that would make bleeding worse. Treatment focuses on stopping the bleed and reducing pressure in the skull. Surgery might be needed:- Coiling: A catheter is threaded up from the groin into the brain. Tiny metal coils are placed inside the aneurysm to block blood flow and prevent re-rupture.
- Clipping: A surgeon opens the skull and places a tiny metal clip on the base of the aneurysm to seal it off. This is still the best option for certain aneurysm shapes and locations.
- Minimally invasive surgery: Newer techniques, like the MISTIE III trial showed, can drain blood with a small tube and use clot-dissolving drugs directly at the site - cutting death rates by 10%.
Prevention: Two Different Playbooks
You can’t prevent all strokes - but you can cut your risk dramatically. And the strategies are different for each type.Preventing Ischemic Stroke
- Manage AFib: If you have atrial fibrillation, you’re five times more likely to have a stroke. Blood thinners like apixaban or rivaroxaban reduce that risk by 60% to 70%. Don’t skip doses.
- Take antiplatelets: Aspirin (81 mg daily) or clopidogrel can lower the chance of a second stroke by 25% if you’ve already had one.
- Control cholesterol: Statins don’t just lower cholesterol - they stabilize plaque in arteries, making clots less likely.
- Don’t smoke: Smoking damages blood vessels and speeds up plaque buildup. Quitting cuts stroke risk in half within one year.
Preventing Hemorrhagic Stroke
- Control blood pressure: This is the #1 thing you can do. The SPRINT trial proved that keeping systolic pressure below 120 mmHg (instead of the old target of 140) cuts hemorrhagic stroke risk by 38%. That’s more than any drug.
- Check for aneurysms: If you have a family history or a history of high blood pressure, talk to your doctor about screening. Not everyone needs it - but some do.
- Avoid heavy alcohol and cocaine: Both raise blood pressure suddenly and can trigger rupture.
- Use anticoagulants carefully: If you’re on blood thinners for AFib, your doctor needs to monitor your levels closely. Too much increases bleeding risk.
Lifestyle Changes That Help Both Types
Some habits protect against all strokes:- The Mediterranean diet: Rich in olive oil, nuts, fish, vegetables, and whole grains. The PREDIMED study showed a 30% drop in stroke risk.
- Move every day: Just 150 minutes of moderate exercise a week - like brisk walking - cuts overall stroke risk by 27%.
- Maintain a healthy weight: Obesity increases inflammation and blood pressure. Losing even 10 pounds helps.
- Get enough sleep: Chronic sleep deprivation raises blood pressure and stress hormones. Aim for 7 to 8 hours.

What to Do If You Suspect a Stroke
Don’t wait. Don’t drive yourself. Call emergency services immediately. Use the FAST test:- Face: Ask them to smile. Does one side droop?
- Arm: Ask them to raise both arms. Does one drift down?
- Speech: Ask them to repeat a simple phrase. Is it slurred or strange?
- Time: If you see any of these signs, call 911 now.
What’s Changing Now?
New tools are making stroke care faster and smarter:- Blood tests: A new biomarker called GFAP can tell if a stroke is hemorrhagic or ischemic within 15 minutes - just from a blood draw. This could help paramedics make better decisions before reaching the hospital.
- AI imaging: Systems like Viz.ai scan CT scans in seconds and alert stroke teams. One hospital reported cutting door-to-needle time by over 50 minutes.
- Extended treatment windows: MRI scans now help doctors identify brain tissue that’s still salvageable, even up to 9 hours after symptoms start. This opens treatment to more people.
Final Thought: It’s Not Just About Age
Most people think stroke only happens to older adults. But 1 in 4 strokes now occur in people under 55. Younger people with untreated high blood pressure, smoking, or undiagnosed AFib are at risk. Prevention isn’t optional - it’s essential, no matter your age. The best defense? Know your numbers - blood pressure, cholesterol, heart rhythm. Talk to your doctor. Make changes. And if someone shows signs of stroke - don’t hesitate. Call 911. Your quick action could mean the difference between recovery and lifelong disability.Can you have a stroke and not know it?
Yes. Small strokes, especially lacunar strokes (tiny clots in deep brain vessels), can cause subtle symptoms like mild memory loss, slight balance issues, or a feeling of "fogginess." These are often dismissed as aging or stress. But repeated small strokes can lead to vascular dementia. If you notice changes in thinking, mood, or movement over time, get checked.
Is aspirin good for preventing stroke?
Aspirin can help prevent a second ischemic stroke, especially if you’ve had one before. But it’s not recommended for everyone as a first-line prevention. For people with no history of heart disease or stroke, the bleeding risk may outweigh the benefit. Always talk to your doctor before starting daily aspirin.
Can stress cause a stroke?
Stress doesn’t directly cause a stroke, but it raises blood pressure, increases inflammation, and can lead to unhealthy habits like smoking or overeating - all of which raise stroke risk. Chronic stress is a silent contributor. Managing stress through sleep, exercise, or therapy is part of stroke prevention.
Are hemorrhagic strokes more dangerous than ischemic?
Yes, in the short term. Hemorrhagic strokes have a higher death rate in the first 30 days - about 23% higher than ischemic strokes, even after accounting for severity. But long-term outcomes depend more on how much brain damage occurred, not just the stroke type. Recovery is possible with intensive rehab, even after a hemorrhagic stroke.
Can you recover fully from a stroke?
Many people do - especially if they get treatment fast. About 10% recover almost completely. Another 25% have minor impairments. About 40% need some help with daily tasks. Recovery takes time, often months or years. Physical therapy, speech therapy, and consistent exercise are key. The brain can rewire itself - but only if you keep working at it.
What should I do if I have high blood pressure?
Get it checked regularly. If it’s over 130/80, talk to your doctor. Lifestyle changes - cutting salt, eating more veggies, walking daily - can lower it. If those aren’t enough, medication works. The goal isn’t just to get it below 140 - aim for under 120 if your doctor says it’s safe. That single change can cut your stroke risk by nearly 40%.
Aisling Maguire
Just read this whole thing during my lunch break and honestly? Mind blown. I had no idea hemorrhagic strokes had that much of a headache difference. My aunt had a stroke last year and they said it was "just a clot" - turns out she had a thrombotic one. I’m gonna send this to her whole family. Also, the part about AFib and blood thinners? My uncle’s on apixaban and he’s been doing great. Seriously, this is the most useful medical post I’ve seen in years.
Sumit Mohan Saxena
The data presented herein is both statistically robust and clinically relevant. The distinction between ischemic and hemorrhagic etiologies is paramount in emergency triage protocols. Furthermore, the SPRINT trial’s findings regarding systolic blood pressure targets below 120 mmHg represent a paradigm shift in preventive neurology. It is imperative that primary care providers adopt these thresholds without delay, as the reduction in hemorrhagic stroke incidence is both statistically significant and clinically actionable.
Jimmy Quilty
so like… i dont trust any of this. i mean, who says the clot is even the problem? what if it’s the *vaccines* that clog your vessels? i read this guy on youtube who said the spike protein sticks to endothelial cells like glue. and then they say "statins stabilize plaque" - but what if plaque is just your body’s way of patching up the damage from the poison in the water? and why do they always skip the part about glyphosate? i’ve been taking magnesium and turmeric and my BP’s down 20 points. they don’t want you to know this.
Miranda Anderson
I’ve been thinking about this a lot since my dad had a mini-stroke last year. I didn’t realize how subtle the signs could be - he just kept saying he felt "off," like his brain was wrapped in cotton. We thought it was stress or aging. Turns out it was a lacunar stroke. This post really hit home. The part about sleep and Mediterranean diet? We switched to olive oil, started walking after dinner, and cut out processed sugar. It’s not a cure, but it’s changed our whole vibe. My mom’s sleeping better. Dad’s more alert. And honestly? I think we’re gonna keep going with this. It’s not about being perfect - it’s about being consistent. Also, the GFAP blood test? That’s wild. I hope it becomes standard soon. No one should have to wait hours for answers.
Gigi Valdez
The clinical distinctions between ischemic and hemorrhagic stroke remain critically important for accurate diagnosis and appropriate intervention. While the FAST mnemonic is widely taught, its sensitivity for hemorrhagic events is not absolute. The inclusion of eye movement abnormalities and agitation as differentiators enhances diagnostic precision. Additionally, the extended treatment window for thrombectomy based on perfusion imaging represents a significant advancement in stroke care delivery. These protocols require multidisciplinary coordination and institutional commitment, which remain unevenly distributed globally.
Sneha Mahapatra
It’s strange how we treat stroke like an emergency, but ignore the slow creep of high blood pressure like it’s just part of getting older. I’ve seen so many people in my community brush off BP readings because "they feel fine." But the brain doesn’t scream before it breaks. It whispers. And we’ve trained ourselves to ignore the whisper. I’m not saying we should panic - but we should listen. The fact that 1 in 4 strokes happen under 55? That’s not luck. That’s neglect. And the silence around it? It’s louder than any headache.
bill cook
Okay but why is everyone acting like this is new info? I’ve been screaming about this since 2019. My cousin died from a hemorrhagic stroke because they gave him tPA. He had no history of clotting, just high BP. They didn’t even scan him first. And now they’re acting like this is groundbreaking? Where was this when my sister was begging for a CT? They don’t care unless it’s trending. Also, the "Mediterranean diet"? That’s just fancy talk for "eat less crap." Why not just say that?
Byron Duvall
Big Pharma wrote this. You know it. They’re pushing this "blood thinner" nonsense because they make billions off it. Meanwhile, the real cause? EMF radiation from 5G towers. I read a paper - it’s in the Journal of Neurotoxicology. They’re covering it up. And don’t even get me started on glyphosate in your oat milk. That’s what’s causing the clots. And why do they always say "call 911"? What if 911 is part of the system? I’d rather drive myself to the clinic and ask for a magnesium IV. That’s what my cousin did. He’s fine now. They just don’t want you to know.
Katherine Farmer
How quaint. A 1500-word essay on stroke types - as if the average person has access to tPA, thrombectomy centers, or even a primary care physician who knows what GFAP stands for. This reads like a textbook written for neurologists in Boston, not someone in rural Alabama. You talk about prevention? Tell me how someone on minimum wage, working two jobs, with no insurance, is supposed to "control BP" or eat Mediterranean food. The real stroke here is the system that lets this disparity exist. This isn’t medicine. It’s a luxury pamphlet.
Full Scale Webmaster
Okay so I’ve been researching this for weeks and I have to say - this is the most comprehensive thing I’ve ever seen. But here’s the thing they don’t tell you: the entire stroke industry is built on fear. Why do you think they push "time is brain" so hard? Because if you panic, you go to the ER. And if you go to the ER, you get scanned, you get a bill, you get a follow-up, you get on lifelong meds. And guess who profits? Hospitals. Pharma. Insurance. I’ve talked to 17 neurologists. Half of them admitted they’d rather have an ischemic stroke than hemorrhagic - because hemorrhagic means you can’t use their fancy clot-busting drugs. And guess what? The "new" AI imaging? It’s just another way to upsell CT scans. The real solution? Stop eating processed food. Stop sitting. Stop stressing. But nobody wants to say that. Because it’s not profitable. And that’s why we’re all just… stuck.
Brandie Bradshaw
I appreciate the depth here - truly - but let’s be brutally honest: we’re still treating stroke like a medical event, not a societal failure. The fact that 795,000 Americans have strokes every year isn’t a statistical anomaly - it’s a policy failure. We have the tools. We have the data. We have the technology. But we don’t have the political will to make blood pressure screening free, to fund community health workers, to regulate food deserts, to enforce workplace wellness. You talk about statins and aspirin - but what about the 40% of Americans who can’t afford their prescriptions? Or the 30% who live in counties with zero stroke centers? This post reads like a luxury brochure for people who already have access. The real prevention isn’t in the brain - it’s in the ballot box.
Lisa Fremder
My mom had a stroke at 48. They said it was "stress." Turns out it was high BP and she was on birth control. I’m 31 now. I check my BP every week. I don’t care what anyone says - this isn’t about age. It’s about awareness. And if you’re not checking your numbers, you’re gambling.