The Journey from Sunlight to Active Hormone
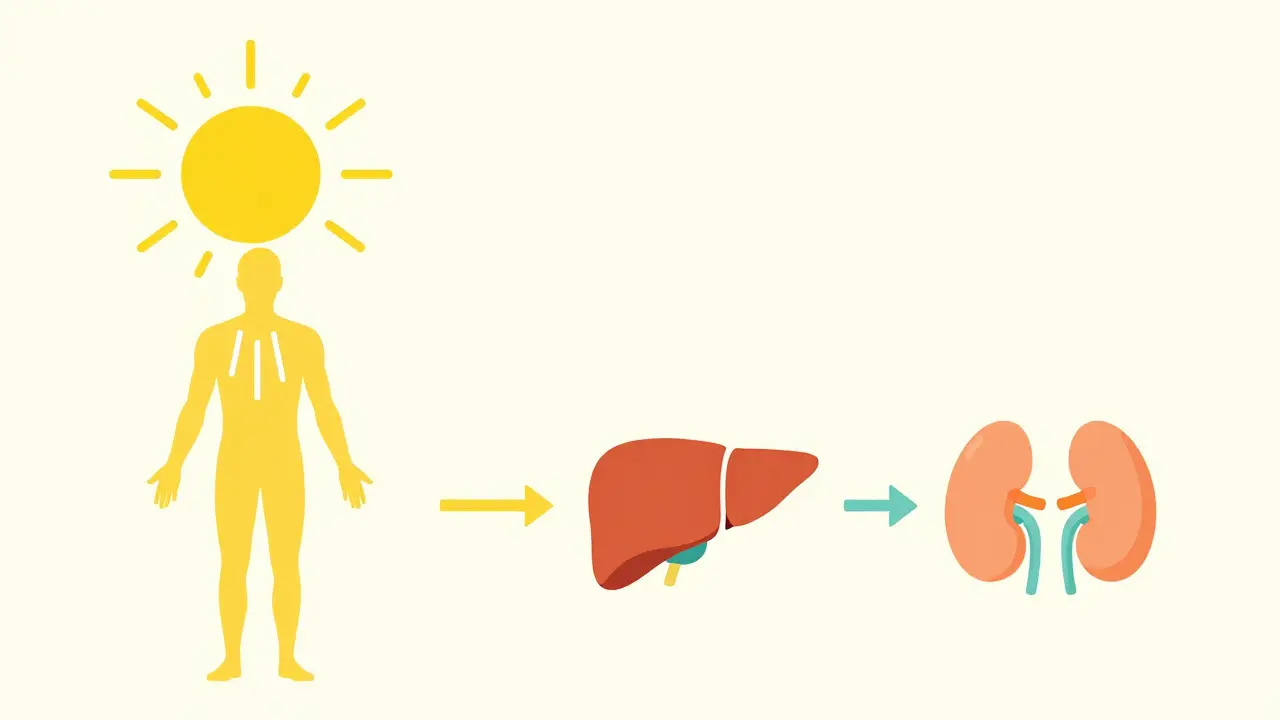
Your body doesn't just "absorb" Vitamin D; it manufactures it through a sophisticated multi-step process. It starts in the skin, where Vitamin D3 (cholecalciferol) is synthesized when your skin hits UVB rays (specifically 290-315 nm). Alternatively, you can get Vitamin D2 (ergocalciferol) from plant sources. Neither of these is actually "active" yet. To become useful, these forms must travel to the liver. Here, the enzyme CYP2R1 converts them into 25-hydroxyvitamin D (25(OH)D). This is the form doctors measure when they order a "Vitamin D test" because it stays in your blood the longest and serves as the best indicator of your overall storage. But the real magic happens in the kidneys. The enzyme CYP27B1 performs a second transformation to create calcitriol (1,25-dihydroxyvitamin D), the biologically active hormone. This final step is tightly controlled by the Parathyroid Hormone (PTH) and calcium levels. If your calcium drops, PTH signals the kidneys to crank out more calcitriol to bring those levels back up.Understanding the Vitamin D Receptor (VDR)
How does a hormone in your blood actually change how a cell behaves? It uses a lock-and-key system. The "lock" is the Vitamin D Receptor (VDR), a nuclear transcription factor found in almost every cell in the human body. When calcitriol binds to the VDR, it enters the cell nucleus and instructs the DNA to turn specific genes on or off. An analysis in Endocrine Reviews (2024) found that the VDR regulates a staggering 11,031 putative target genes. It isn't just about bones. About 43% of these genes are involved in metabolism, 19% in how tissues are shaped, and 9% in angiogenesis (the growth of new blood vessels). This explains why Vitamin D is linked to so many different health outcomes beyond just skeletal strength.
Endocrine vs. Autocrine: The Great Paradox
This is where things get interesting. There are two ways Vitamin D works in your body: the systemic (endocrine) path and the local (autocrine) path.| Feature | Endocrine Pathway (Systemic) | Autocrine Pathway (Local) |
|---|---|---|
| Primary Goal | Maintain blood calcium levels (8.5-10.5 mg/dL) | Modulate local gene expression and cell function |
| Activation Site | Primarily the kidneys | Local tissues (immune cells, skin, prostate) |
| Speed of Action | Rapid (minutes to hours) | Slower, long-term cellular changes |
| Key Regulators | PTH, FGF23, Serum Calcium | Local inflammatory signals, infection |
The Realities of Supplementation: Dosing and Pitfalls
If you're looking to improve your levels, you can't just take a random dose and hope for the best. The amount you need depends heavily on your biology. For most adults under 70, the Endocrine Society suggests 600-2,000 IU per day. However, that number changes based on a few critical factors:- Body Mass Index (BMI): Vitamin D is fat-soluble, meaning it gets sequestered in adipose tissue. People with obesity (BMI ≥30) often need 2-3 times the standard dose. In some studies, 3,000 IU was required to reach the same target that 1,500 IU achieved in a lean person.
- Absorption Issues: If you have celiac disease or other malabsorption syndromes, your gut can't move Vitamin D into the bloodstream efficiently. You might need higher daily doses or intermittent high-dose regimens (like 50,000 IU weekly) to overcome this barrier.
- The Lag Time: Don't retest your blood two weeks after starting a supplement. Serum 25(OH)D levels usually lag behind supplementation by 2-3 months.
The Great Debate: Does it Actually Prevent Disease?
There is a massive rift in the medical community regarding Vitamin D. On one side, experts like Dr. Michael Holick argue that deficiency contributes to type 2 diabetes and cardiovascular disease, citing epidemiological data showing a 30-50% higher risk in people with levels below 20 ng/mL. On the other side, the VITAL trial-one of the largest studies of its kind with over 25,000 participants-found that 2,000 IU of D3 daily didn't significantly reduce major cardiovascular events or invasive cancers. This discrepancy suggests that while Vitamin D is absolutely essential for bone health and calcium balance, using it as a "cure-all" preventive for other diseases might be overreaching.Looking Ahead: Targeted Analogs and Personalized Medicine
We are moving away from a one-size-fits-all approach. The future isn't just about taking a pill; it's about targeting specific receptors. For instance, pharmaceutical companies are developing analogs like VDRM-110 that target pancreatic beta cells to help with insulin secretion without causing the high calcium levels that native Vitamin D can trigger. We are also learning that genetics play a huge role. Variations in the Vitamin D Binding Protein (DBP) determine how much "free" hormone is actually available to your cells. Two people could have the exact same blood test result, but one might have more biologically active free hormone than the other due to their DBP genotype.What is the difference between Vitamin D2 and D3?
Vitamin D2 (ergocalciferol) is derived from plants and fungi, while Vitamin D3 (cholecalciferol) is synthesized by the skin upon exposure to UVB sunlight or obtained from animal sources. D3 is generally considered more effective at raising and maintaining serum 25(OH)D levels over the long term.
Can I take too much Vitamin D?
Yes. While rare, excessive supplementation (typically >4,000 IU daily over long periods) can lead to hypercalcemia, where calcium builds up in the blood. This can cause nausea, weakness, and in severe cases, kidney stones or heart rhythm issues. Toxicity is generally seen at serum levels above 150 ng/mL.
Why do my blood levels stay low even though I take supplements?
There are several reasons. First, Vitamin D is fat-soluble, so you should take it with a meal containing fat for better absorption. Second, if you have a high BMI, the vitamin may be sequestered in fat tissue. Third, genetic polymorphisms in the CYP2R1 enzyme can make some people less efficient at converting the supplement into its circulating form.
Do I really need a blood test to start supplementing?
For most healthy adults, a modest dose (600-1,000 IU) is generally safe. However, the Endocrine Society recommends testing for high-risk groups: people with osteoporosis, chronic kidney disease, or malabsorption syndromes (like celiac disease), where deficiency rates can range from 35% to 90%.
How long does it take for Vitamin D supplements to work?
While some people report feeling improvements in fatigue or muscle weakness within a few weeks, serum levels of 25(OH)D typically take 2 to 3 months of consistent supplementation to reach a new steady state. You should wait at least this long before re-testing your levels.
Jarrett Jensen
The author's presentation is adequate, yet one cannot help but notice the superficial treatment of the VDR polymorphisms. It is profoundly simplistic to suggest that BMI is the primary hurdle for absorption without discussing the nuanced interplay of the cytochrome P450 enzymes in greater detail. One would expect a more rigorous academic approach to the synthesis pathways if the intent was to truly educate the sophisticated reader. Frankly, the juxtaposition of epidemiological data against the VITAL trial lacks the necessary critical synthesis to be considered a comprehensive analysis. It is merely a curated summary for the layperson, lacking the intellectual rigor required for genuine endocrine discourse.
Amber McCallum
Most people just take pills and think they are fixed. You have to realize that your mind and spirit need to be aligned with your health or the vitamins do nothing. It's just basic logic.
Timothy Brown
Listen, if you're not taking your D3 with a fat source, you're basically flushing money down the toilet. I've seen so many people fail at this because they ignore the basics of fat-solubility. Stop guessing and start doing it right.
Peter Minto
usa made vitamins are the only ones that matter!! dont trust those importd ones from god knows where they probably put lead in them lol. why do people even buy foreign stuff when we got the best labs in the world right here!!
Kali Murray
interesting read ☁️ definitely helpful to know about the lag time for blood tests
Kevin Taggart
i didnt know about the kidney part... thots its just skin and liver :)
Darrin Oneto
That autocrine stuff is total wizardry man. Its like haveing a secret lab in every single cell just waitin for a signal to go ham on a virus. Absolute madness how the body rolls 🤘
Jonathan Hall
While I generally strive to maintain a peaceful dialogue regarding our divergent health philosophies, I must insist that the blatant disregard for the traditional dietary approaches found in other cultures is an aggressive oversight in this text, as those who embrace a more holistic, global perspective on nutrition often find that the synthetic supplementation mentioned here is a clumsy, blunt instrument compared to the elegant synergy of a naturally sourced, culturally diverse diet that has sustained populations for millennia without the need for pharmaceutical analogs that often strip away the essential co-factors required for true systemic harmony.