When you take an antiplatelet medication like aspirin, clopidogrel, or ticagrelor, you're doing more than just swallowing a pill. You're lowering your chance of a heart attack or stroke by stopping your blood from clotting too easily. But there's a trade-off: your stomach becomes more vulnerable. Antiplatelet medications are lifesavers for millions, but they also increase the risk of serious gastrointestinal bleeding-sometimes without warning.
Why Antiplatelet Drugs Put Your Stomach at Risk
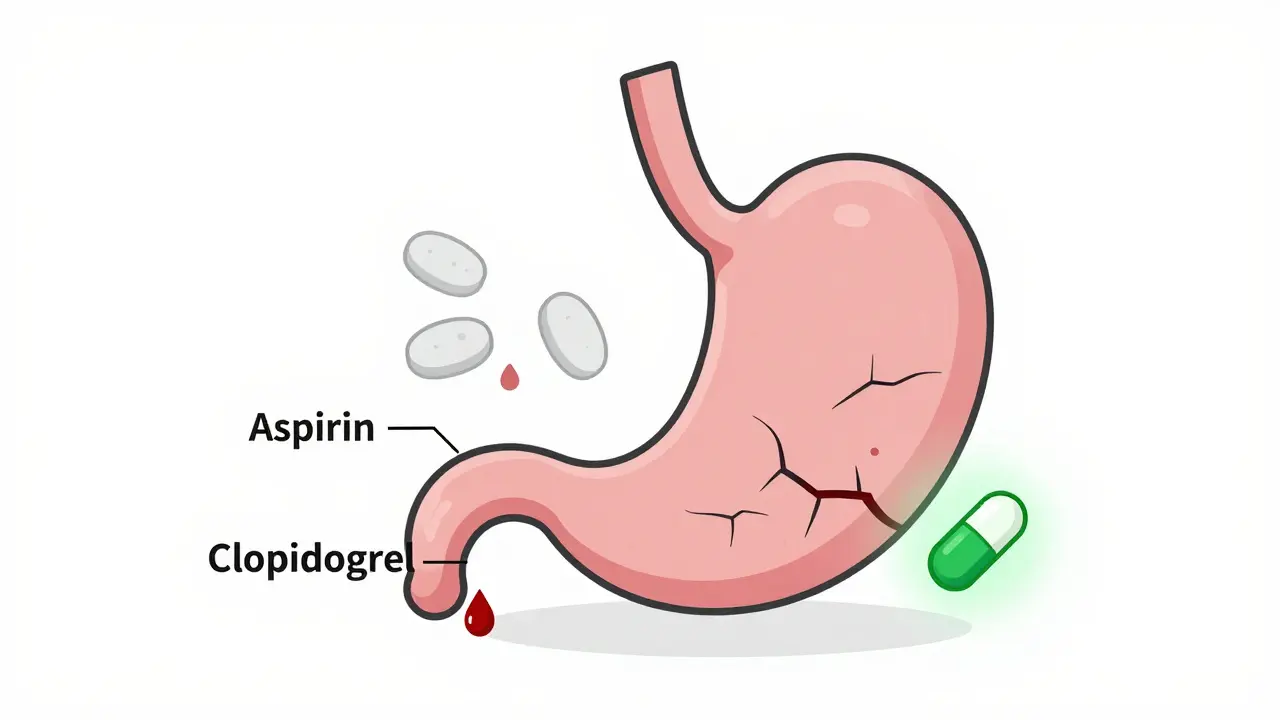
Antiplatelet drugs work by blocking platelets, the tiny blood cells that help clots form. That’s good for your arteries, but bad for your stomach lining. Your stomach needs platelets to repair tiny cuts that happen every day from stomach acid and food. When these drugs are active, those cuts don’t heal. Over time, they turn into ulcers. And ulcers can bleed-sometimes heavily. Aspirin is the oldest and most common. It’s been used for decades to prevent heart disease. But even enteric-coated aspirin doesn’t protect your stomach. The coating only delays when the drug dissolves; it doesn’t stop the antiplatelet effect. Once aspirin enters your bloodstream, it keeps platelets from working for the rest of their 7-10 day life. That means no repair work on your stomach lining. P2Y12 inhibitors like clopidogrel, prasugrel, and ticagrelor are stronger. They block a different pathway in platelets and are often used after stents or heart attacks. But they’re also more likely to cause bleeding. Studies show clopidogrel raises the risk of gastrointestinal injury by 80% compared to aspirin alone. Prasugrel and ticagrelor? Even higher. Ticagrelor increases bleeding risk by 30% over clopidogrel, according to the PLATO trial. Dual therapy-taking two antiplatelet drugs at once-is common after stent placement. But it doubles the risk. About 1 in 100 people on dual therapy will have noticeable bleeding within the first month. And over 6-12 months, up to half of those on clopidogrel or dual therapy show signs of ongoing stomach damage, even if they feel fine.Who’s Most at Risk?
Not everyone on antiplatelets will bleed. But some people are far more vulnerable:- People over 65
- Those with a history of ulcers or GI bleeding
- Patients taking NSAIDs (like ibuprofen or naproxen) at the same time
- People with H. pylori infection
- Those on blood thinners like warfarin or apixaban
- Patients with low albumin, high INR, or low blood pressure
Protecting Your Stomach: The Role of PPIs
Proton pump inhibitors (PPIs) like omeprazole, esomeprazole, and pantoprazole are the go-to solution. They reduce stomach acid, letting ulcers heal and preventing new ones. Studies show PPIs cut the risk of GI bleeding in half for people on antiplatelet therapy. The American College of Gastroenterology recommends PPIs for:- Anyone with a past history of GI bleeding
- Patients on dual antiplatelet therapy
- Those over 65 taking aspirin or clopidogrel
- People also using NSAIDs or steroids
The Clopidogrel-PPI Interaction Myth
You’ve probably heard that PPIs interfere with clopidogrel. It’s a big concern, especially among cardiologists. The idea is that PPIs block an enzyme (CYP2C19) that turns clopidogrel into its active form. Less activation = less protection = higher risk of heart attack. But here’s the truth: studies are mixed. A 2010 FDA review found the clinical impact uncertain. A 2023 meta-analysis of 15 trials showed no significant increase in heart attacks or death when PPIs were used with clopidogrel. Meanwhile, the risk of bleeding dropped sharply. Most experts now agree: if you need a PPI for stomach protection, take it. The bleeding risk is real. The heart attack risk from skipping a PPI is higher than the risk from the interaction. If you’re worried, take your PPI at night and your clopidogrel in the morning. That’s enough separation for most people.What to Do If You Bleed
If you notice black, tarry stools, vomit blood, or feel dizzy and weak, get help immediately. But don’t stop your antiplatelet medication on your own. The 2023 guidelines are clear: do not stop aspirin during GI bleeding. Stopping it increases death risk by 25%. Aspirin is so critical for preventing clots that even during active bleeding, doctors often keep it going. For clopidogrel, prasugrel, or ticagrelor, hold them for 5-7 days if bleeding is active. But restart as soon as possible. Delaying too long raises the risk of stent clotting. One study found 3 patients had heart attacks within 30 days of stopping clopidogrel because they were scared of stomach bleeding. Platelet transfusions? Don’t do them. A 2023 study showed patients who got transfusions during GI bleeding had nearly double the death rate. Platelets don’t help here-they can make clots worse.
What’s Next? The Future of Safer Antiplatelets
Researchers are working on new drugs that protect the heart without hurting the stomach. Selatogrel, currently in Phase III trials, shows promise. In early studies, it caused 35% less stomach injury than ticagrelor. That’s huge. Another path is personalized medicine. Some people don’t respond to clopidogrel because of their genes (CYP2C19 mutations). Testing for these mutations could help doctors choose better drugs upfront. One day, a simple blood test might tell you: “You should take ticagrelor, not clopidogrel, because your body can’t activate it well-and you’re at high risk for bleeding.” Right now, the best strategy is simple: know your risk. Talk to your doctor about your stomach history, other meds, and age. If you’re on dual therapy or over 65, ask about a PPI. Don’t skip it because of fear of interactions. The data is clear: protection wins.Real Talk: What Patients Are Saying
A survey of 1,247 gastroenterologists found 89% routinely prescribe PPIs to patients with prior ulcers. And it works. In one case series, 92% of patients on clopidogrel who took esomeprazole had their ulcers fully healed in 8 weeks. But confusion is common. One Reddit thread from May 2023 had 147 comments from doctors. Many shared stories of patients quitting clopidogrel because of stomach pain-only to end up back in the ER with a stent clot. Others worried about long-term PPI use. “I’m scared of bone loss and kidney damage,” one patient wrote. But the risk of bleeding without a PPI is far higher. The bottom line? Antiplatelet therapy saves lives. But it’s not harmless. The goal isn’t to avoid the medication. It’s to manage the risk.Can I stop my antiplatelet medication if I have stomach bleeding?
No, don’t stop aspirin. Stopping it increases your risk of death by 25%. For other antiplatelets like clopidogrel or ticagrelor, your doctor may ask you to pause them for 5-7 days during active bleeding, but they’ll want you to restart as soon as it’s safe. Delaying too long can cause a deadly clot in your stent.
Do PPIs make clopidogrel less effective?
The concern exists, but real-world evidence doesn’t support it. Early studies suggested a possible interaction, but large reviews and clinical trials since 2017 show no increase in heart attacks or death when PPIs are used with clopidogrel. The benefit of preventing life-threatening bleeding outweighs the unproven risk of reduced effectiveness. If you’re concerned, take your PPI at night and clopidogrel in the morning.
Is enteric-coated aspirin safer for my stomach?
No. The coating only delays how fast aspirin dissolves in your stomach. Once absorbed into your bloodstream, it still blocks platelets everywhere-including your stomach lining. It doesn’t reduce bleeding risk. If you’re at risk for GI bleeding, you still need a PPI, even if you take enteric-coated aspirin.
Should I take a PPI if I’m on aspirin only?
It depends. If you’re over 65, have a history of ulcers, take NSAIDs, or have other risk factors, yes. For healthy people under 65 on low-dose aspirin with no prior GI issues, a PPI isn’t usually needed. But if you’ve ever had bleeding, even once, you should be on a PPI long-term.
What are the long-term risks of taking PPIs?
Long-term PPI use (over a year) can slightly increase the risk of low magnesium, bone fractures, or kidney issues-but these are rare. The risk of a major GI bleed from stopping a PPI is far greater. For most people on antiplatelets, the benefits of preventing bleeding outweigh the small long-term risks. If you’re on a PPI for years, have your doctor check your kidney function and magnesium levels every 1-2 years.
Kevin Y.
Just wanted to say this post is incredibly well-structured and clinically accurate. As a cardiologist, I see patients every week who stop their meds because they’re scared of stomach issues-and then end up back in the ER with a clot. The PPI data is solid. If you’re over 65 or on dual therapy, take the PPI. No debate. The bleeding risk without it is real, and the interaction myth has been debunked by multiple large trials. Don’t let fear override evidence.
winnipeg whitegloves
Man, this is the kind of post that makes me feel like I’m reading a medical thriller instead of a blog. Antiplatelets are like that one friend who’s always there for you at the party-but they also keep knocking over your favorite vase. PPIs? The trusty napkin you keep in your pocket. Sure, it’s not glamorous, but you’ll be glad you’ve got it when things get messy. Also, enteric-coated aspirin is just aspirin in a fancy coat. Doesn’t fool your stomach.
Marissa Staples
I think about how our bodies are just these fragile systems trying to balance survival and self-destruction. We take these drugs to keep our hearts from failing, but they quietly erode our stomachs like time erodes a cliff. Is it worth it? Yes. But we should be more honest about the cost. The body doesn’t lie-it bleeds. And yet we keep pushing pills because we’re afraid of dying more than we’re afraid of the slow unraveling. Maybe we need to grieve the trade-offs, not just accept them.
Rachele Tycksen
i just took asprin for my headache and now im scared i m gonna bleed out from my stomach lol
Grace Kusta Nasralla
I used to think medicine was about healing… but now I see it’s mostly about managing the slow collapse of the body. We patch one hole with a drug, and it tears another. PPIs? A temporary bandage on a wound we refuse to stop making. I wonder if we’re just delaying the inevitable-feeding our fear of death while ignoring how we’re slowly killing ourselves with the very things meant to save us.
Korn Deno
PPIs work. Period. Don't overthink it. If you're on dual therapy or over 65 you need it. The interaction with clopidogrel is a ghost story doctors tell to scare patients. Real data says no significant risk. Take the pill. Sleep better. Live longer.
Aaron Sims
Okay, so let me get this straight… the FDA, the ACG, and every cardiologist in the country are telling you to take a PPI… but the REAL truth is that Big Pharma is secretly using this to sell more proton pumps? I mean, think about it-PPIs have been on the market for 30 years, and suddenly everyone’s bleeding? Coincidence? Or is this just a multi-billion-dollar distraction so we don’t ask why we’re all on 7 different pills just to stay alive? I’m not saying it’s wrong-I’m just saying… who profits?
Stephen Alabi
While the majority of the information presented here is factually accurate, it is critically incomplete. The 2023 meta-analysis referenced does not account for the heterogeneity in CYP2C19 loss-of-function allele prevalence across ethnic populations. East Asian populations, for example, demonstrate a 50% higher rate of non-response to clopidogrel. Furthermore, the recommendation to continue aspirin during active GI bleeding is based on a single retrospective cohort study with significant confounding variables-including concomitant NSAID use and failure to stratify by bleeding severity. The true mortality benefit of continuing aspirin remains unproven in randomized controlled trials. Additionally, long-term PPI use has been associated with small intestinal bacterial overgrowth (SIBO), which may contribute to chronic inflammation and increased cardiovascular risk-something entirely omitted here. This post is dangerously oversimplified.